
Understanding Gleason Grading
Introduction |
The five Gleason grades |
The combined Gleason score or Gleason sum |
What does the Gleason score mean?
Introduction
Physicians use the term "grade" to describe the appearance of thin slices of cancer tissue when it is
observed under a microscope. In the case of prostate cancer tissue, the most common system used in
the USA to grade the appearance of this tissue is called the Gleason grading system, after the
physician who first described this system.
The Gleason grading system is not the only grading system in use around the world. However,
because it is the one most commonly used in the USA, it is the one we will try to explain here. If
your physician talks to you about the grade of your prostate cancer, you may want to ask if it is the
Gleason grade that he or she is referring to.
The Gleason grade is one of several pieces of information determined by
the pathologist who examines the biopsy specimen taken from the prostate.
Readers wishing to understand more about the role of the pathologist in
the diagnosis of prostate cancer may wish to read the article entitled
"The pathologic examination of prostate tissue",
which addresses this topic in detail, and which also explains the importance to the
patient of receiving a copy of his pathology report.
The Gleason system is based exclusively on the architectural pattern of the glands of the prostate
tumor. It evaluates how effectively the cells of any particular cancer are able to structure themselves
into glands resembling those of the normal prostate. The ability of a tumor to mimic normal gland
architecture is called its differentiation, and experience has shown that a tumor whose structure is
nearly normal (well differentiated) will probably have a biological behavior relatively close to normal
-- that is not very aggressively malignant.
The principle is fairly simple, and Gleason grading from very well differentiated (grade 1) to very
poorly differentiated (grade 5) is usually done for the most part by viewing the low magnification
microscopic image of the cancer. There are important additional details which require higher
magnification, and an ability to accurately grade any tumor is achieved only through much training
and experience in pathology.
The five Gleason grades
Dr. Gleason has provided a conceptual diagram (oversimplified) in Figure 1 to show
the continuum of deteriorating cancer cell architecture, and the four dividing lines along this
continuum which he discovered are able to identify patients with significantly different prognosis
derived from a study which included 2,900 patients.
Figure 1: This illustration shows Dr. Gleason's
own simplified drawing of the five Gleason grades of prostate cancer.
Grade 1 appears on the far left and grade 5 on the far right. Adapted
from Gleason DF. The Veteran's Administration Cooperative Urologic
Research Group: histologic grading and clinical
staging of prostatic
carcinoma. In Tannenbaum M (ed.) Urologic Pathology: The Prostate. Lea
and Febiger, Philadelphia, 1977;
171-198.
In the illustrations and text that follow, we have given real examples of tissues which show the five
Gleason grades and tried to describe the differences between them. We would like to thank Dr John
McNeal of the Department of Urology, Stanford University School of Medicine, for kindly providing
these illustrations and assisting us in developing this information.
- Gleason Grades 1 and 2:
These two grades closely resemble normal prostate. They are the least important grades because they seldom occur in the general population and because they confer a prognostic benefit which is only slightly better than grade 3. Both of these grades are composed by mass; in grade 2 they are more loosely aggregated, and some glands wander (invade) into the surrounding muscle (stroma).

Figure 2: Grade 1 (left) and grade 2 (right) prostate adenocarcinoma. Both have pale cells and well
formed, separate glands with lumens. Grade 1 is more compact (less invasive) than grade 2.
Illustration courtesy of John E. McNeal, MD, Department of Urology, Stanford University School of Medicine.
- Gleason Grade 3: This is the most common grade by far and is also considered well
differentiated (like grades 1 and 2). This is because all three grades
have a normal "gland unit" like that of a normal prostate; that is, every
cell is part of a circular row which forms the lining of a central space
(the lumen). The lumen contains prostatic secretion like normal
prostate, and each gland unit is surrounded by prostate muscle which
keeps the gland units apart. In contrast to grade 2, wandering of glands
(invading) into the stroma (muscle) is very prominent and is the main
defining feature. The cells are dark rather than pale and the glands
often have more variable shapes. Figure 3
shows invasion under low
magnification; Figure 4 is part of the same area at higher magnification and
shows the separate gland units and the dark cells.
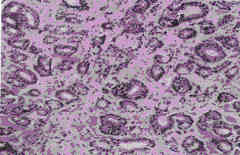
Figure 3: Grade 3 carcinoma with individual glands arranged randomly (invading), seen at low
magnification.
Illustration courtesy of John E. McNeal, MD, Department of Urology, Stanford University School of Medicine.
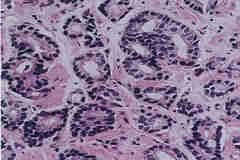
Figure 4: Grade 3 carcinoma (same as shown in Figure 3) showing the usual single layer of cells
around each lumen and showing almost all glands separated by muscle (stroma), seen at higher
magnification.
Illustration courtesy of John E. McNeal, MD, Department of Urology, Stanford University School of Medicine.
- Gleason Grade 4: This is probably the most important grade because it is fairly common
and because of the fact that if a lot of it is present, patient prognosis is
usually (but not always) worsened by a considerable degree. Here also
there is a big jump in loss of architecture. For the first time, we see
disruption and loss of the normal gland unit. In fact, grade 4 is
identified almost entirely by loss of the ability to form individual,
separate gland units, each with its separate lumen (secretory space).
This important distinction is simple in concept but complex in
practice. The reason is that there are a variety of different-appearing
ways in which the cancer's effort to form gland units can be distorted.
Each cancer has its own partial set of tools with which it builds part of
the normal structure. Grade 4 is like the branches of a large tree,
reaching in a number of directions from the (well differentiated) trunk
of grades 1, 2, and 3. Much experience is required for this diagnosis,
and not all patterns are easily distinguished from grade 3. Figure 5
and Figure 6
show two such patterns. This is the main class of
poorly differentiated prostate cancer, and its distinction from grade 3 is
the most commonly important grading decision.
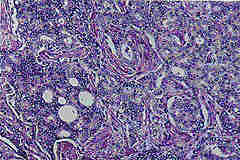
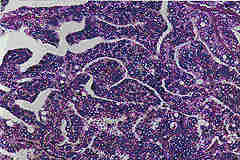
Figure 5 (left) and Figure 6 (right): Grade 4 carcinomas with two different architectural patterns, each of which has lost
the expression of complete "gland units," seen at higher magnification. There are sheets of cells with
randomly scattered lumens.
Illustrations courtesy of John E. McNeal, MD, Department of Urology, Stanford University School of Medicine.
- Gleason Grade 5: Gleason grade 5 is an important grade because it usually predicts
another significant step towards poor prognosis. Its overall importance
for the general population is reduced by the fact that it is less common
than grade 4, and it is seldom seen in men whose prostate cancer is
diagnosed early in its development. This grade too shows a variety of
patterns, all of which demonstrate no evidence of any attempt to form
gland units. Figure 7
shows only a sea of black nuclei with no pattern. The
variety of different appearances is less than for grade 4 because there
are fewer ways to do nothing! This grade is often called
undifferentiated, because its features are not significantly distinguishing
to make it look any different from undifferentiated cancers which
occur in other organs.
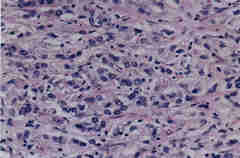
Figure 7: Grade 5 adenocarcinoma, consisting of sheets of cells whose lack of pattern in nuclear
arrangement indicates total loss of architecture, seen at higher magnification.
Illustration courtesy of John E. McNeal, MD, Department of Urology, Stanford University School of Medicine.
If you are interested in seeing other examples of samples showing Gleason grades, try looking at the materials
from the University of Pittsburgh Medical Center.
The combined Gleason score or Gleason sum
When a pathologist looks at prostate cancer specimens under the microscope and gives them a Gleason
grade, he or she in fact will always try to identify two architectural patterns and assign a Gleason
grade to each one. There may be a primary or most common pattern and then a secondary or second
most common pattern which the pathologist will seek to describe for each specimen; alternatively,
there may often be only a single pure grade.
In developing his system, Dr Gleason discovered that by giving a combination of the grades of the two
most common patterns he could see in any particular patient's specimens, he was better able to predict
the likelihood that that particular patient would do well or badly. Therefore, even though it may seem
confusing, the Gleason score which a physician usually gives to a patient is actually a combination or
sum of two numbers. These combined Gleason sums or scores may be determined as follows:
- The lowest possible Gleason score is 2 (1 + 1), where both the primary and secondary
patterns have a Gleason grade of 1 and therefore when added together their combined
sum is 2.
- Very typical Gleason scores might be 5 (2 + 3), where the primary pattern has a
Gleason grade of 2 and the secondary pattern has a grade of 3, or 6 (3 + 3), a pure
pattern.
- Another typical Gleason score might be 7 (4 + 3), where the primary pattern has a
Gleason grade of 4 and the secondary pattern has a grade of 3.
- Finally, the highest possible Gleason score is 10 (5 + 5), when the primary and
secondary patterns both have the most disordered Gleason grades of 5.
What does the Gleason score mean?
The grade of a prostate cancer specimen is very valuable to doctors in helping them to understand how
a particular case of prostate cancer can be treated. In general, the time for which a patient is likely to
survive following a diagnosis of prostate cancer is related to the Gleason score. The lower the
Gleason score, the better the patient is likely to do.
However, remember that prostate cancer is a very complicated disease. People with low Gleason
scores have been known to fare poorly and men with high Gleason scores have been known to do
well. General principles do not always apply to individual patients.
By combining the patient's Gleason score with his PSA level and the clinical
stage estimated by the physician, it is possible to use the
Partin coefficient tables to estimate the likelihood that that patient
has localized or locally advanced prostate cancer of different types.
|
|